Introduction: oncological treatment has been the focus and hotspot of modern medical research. The pattern of the global oncology market is undergoing a considerable shift, and, as new technology becomes available, a large number of patients have more treatment options, which is also redefined in the narrow sense of cancer. However, the traditional treatment of tumours: chemotherapy, decomposition and its large differences in the treatment of patients with tumours, such as single clone antibodies, small molecular inhibitors and high relapse rates, are facing serious challenges. The flourishing of modern immunotherapy has opened new paths to new combination treatments for tumors。
1. Information on treatment for oncology
Tumours are new organisms that are formed as a result of abnormal growth and fragmentation as a result of the loss of normal regulation of the growth of local tissue cells at the genetic level as a result of various tumour-induced factors. Once a new organism is formed, it does not stop growing because of the disease's elimination and its growth is not regulated by the normal body's physiological structure, but rather destroys normal tissues and organs, which is particularly evident in the case of malignant tumours. Compared to benign tumours, malignant neoplasms grow rapidly, immersively, prone to haemorrhage, necrosis, ulcer, etc., and often move far away, resulting in loss of human wasting, infirmity, anaemia, appetite, fever and severe defilement, resulting in death。
Traditional tumour treatment is based on surgery, treatment and chemotherapy. Over the past year, monoclon antibodies, small molecular inhibitors, etc., have developed in the treatment of patients on tumours. However, since many cases of tumours are hidden and early symptoms are not visible, it is difficult to detect them in the early stages of the disease, they are mostly diagnosed in the middle and late stages, they are ineffective, they vary widely, they have a low survival rate over five years, they have a high relapse rate and they are facing serious challenges. In the case of pancreas cancer, which has been recognized as “the king of cancer” as a malignant tumour in the digestive tract as a result of diagnostic difficulties, poor prognosis and high rates of death, only about 7. 5 per cent of patients have been able to survive for more than five years. However, in clinical work, many cases of pancreas cancer face untreated and untreated conditions. Medicine treatment, including chemotherapy, molecular targeting treatment, chinese medicine and support for treatment for the disease, can only be an important appeasement for advanced pancreas cancer. The diversity of genetic information has led to wide disparities in the incidence and efficacy of neoplasms, both in traditional and now emerging treatments, and to high rates of relapse. The flourishing of modern immunotherapy has opened new paths to new combination treatments for tumors。

2. What do you know about immunotherapy
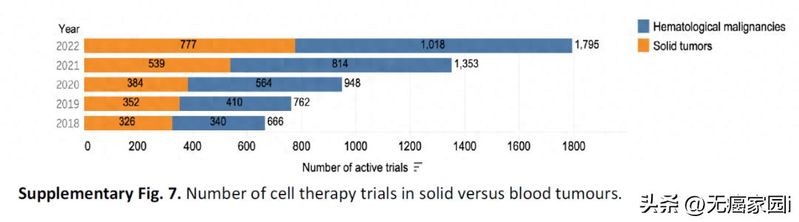
Oncological immunisation treatment is the application of immunological principles and methods to increase the immunoplasia and sensitivity of tumour cells to the effects of cytocinism, to stimulate and enhance the response of the body to tumour immunity, and to apply the immunosuppressive cells and the effector inoculation of the body's immune system to kill tumours and inhibit their growth. Cell immunisation treatment, including tree tattered cell (dc) treatment and embedded antigen receptor t-t (car-t) treatment, has the potential to achieve good clinical results over the next few years through a combination of methods。
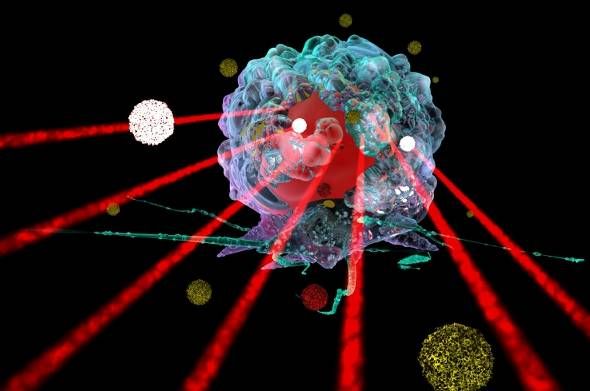
Immunotherapy can isolate t-cells from cancer patients, use genetic engineering in in vitro to modify the modified t-cells to recognize the cancer cells and activate the t-cells, and then transfer them back to the patient after expansion. These modified t-cells (car-t) can quickly locate and react to tumor cells and eventually kill them。
Although tumour immunisation treatment is the current development hotspot in the field of tumours, tumour immunisation treatment is not a new topic. Almost 100 years ago, when immunology was created, scientists developed ideas and made various attempts to use the body's own immune function to attack tumor cells. From 1950s to the present, immunotherapy has continued to develop, and in 2011, the first single resistance to immunosuppression (anti-ctla-4, ipilimumab) was approved by the united states fda for second-line treatment of late-stage melanoma, marking a new era in tumour immunization. Immunotherapy has proven to be a good treatment for cancers such as lung cancer, melanoma and so forth, but immunotherapy has been helpless for pancreas. In july, however, a research team from the washington university school of medicine completed this breakthrough, proving that using routine chemotherapy and immunotherapy for pancreas cancer is a new treatment model, and that the fak inhibitor plus chemotherapy plus immunotherapy “three-pronged” approach is capable of combating cancer in a variety of ways, disrupting its micro-environment-enrichment immune system, and the effect of chemotherapy on on oncological tissue. In recent years, advances in research into new molecules and immunology have provided a good basis for t-cell therapy, and through good design of car-t, optimization of t-cell production and good pre-treatment methods for patients, these advances are opening new avenues for joint treatment of new tumours。
3. Immunotherapy provides new thinking for oncology treatment
T-cell immunisation treatment was for the first time applied to human tumours by the donor's lymphocytes (dli), used for a re-emergenced marrow transplanted blood tumour patient, and further studies have shown that an amplified tumour impregnated cell (til) can provide a complete and sustained mitigation of large vascular transferive melanoma and circulatory tumour cells in the blood. Monitoring by the ctc also shows clinical results of act treatment. Scientists now focus on genetically engineered t-cell technology, which uses retrovirals or particle carriers to modify them, to attack oncular cells by targeting large numbers of t-cells (cart or tcrt). The integration of genetic engineering with immunotherapy has resulted in the provision of genes and the re-entry of in vitro synthetic immunocellular cells using techniques such as pcr. Immunotherapy is a very promising cancer treatment at present, but it is important to explore in depth the factors that explain the resistance of tumours to immunisation treatment, which are still not completely eliminated。
The fight against tumours is a difficult battle, and immunotherapy is the special forces sent by scientists, which play a key role in this battle with special training (cik, cart, til, etc.). Immunization therapy has ushered in an era of innovative changes in the field of immuno-tumours, and will provide significant opportunities in the future。