
Shanghai medical centre for children
Introduction
Pediatric pulmonary artery (ph) is a complex multi-source disease. Various current studies have identified ph as a risk factor for the incidence of complications and increased mortality during heart catheters and non-heart surgery in children. In order to identify factors associated with paediatric ph and serious clinical malpractices to assist clinicians in stratuming risks, researchers such as stein at the boston children's hospital, after obtaining approval from the agency review committee, collected data on all patients under 18 years of age diagnosed with ph from 2015 to 2018 in the electronic medical records and subjected to a heart tube examination, and performed a retrospective analysis. This paper will introduce its publication in june 2022 in journal of cardiothoracic and vascular anthesia, entitled “anthesia in children with pulmo”I'm sorry, but i'm sorry, but i'm sorryThe results of the study by ncardiac procedures。
Methodology
From 2015 to 2018, children with ph who were subjected to heart catheter tests under paediatric anesthesia/aesthetic and guardianship were included in the study. The inclusion criteria meet at least one of the following: an increase in lung vascular resistance (>3 wood unit); an increase in average pulmonary arterial pressure (>25 mmhg); an ph treated with an vascular expansion, and a pericardial interocular pressure difference of >6 mmhg (without pulmonary arterial pressure). (c) excludes children who, through cmri, ct or cardiac catheters, determine that the main pulmonary artery is the main source of lung blood flow。
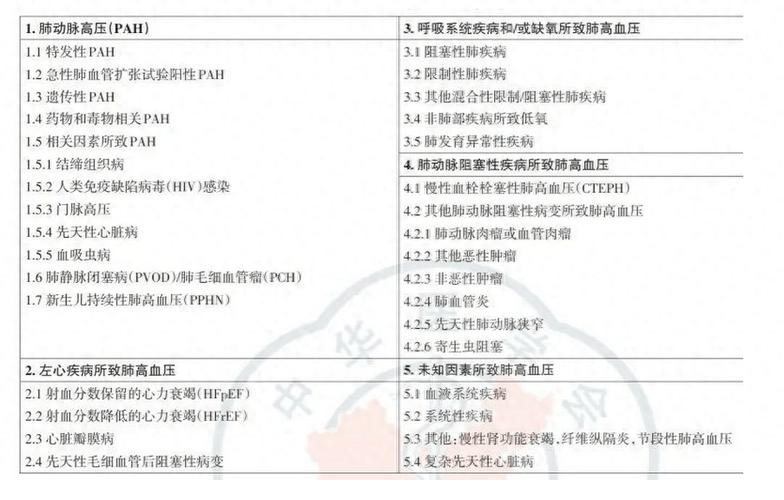
Ph causes are documented according to the description of the medical history and guided by the panama pulmonary artery high pressure standard. Ph due to various causes is recorded separately in each category. Retrospect the latest ultrasound map before the heart catheter examination. Dismissal of patients aged 18 or over who have lost ph after heart, lung or subsequent heart catheter examination。
The records contain data from each of the first and subsequent catheters conducted under the supervision of the paediatric anesthetist. According to the main anesthesia methods, patients are classified into three categories: inhalation of anaesthesia (hexafluorine or hexafluoroane), entirely by intravenous anesthesia, or only by oral or muscle injection. The management of the airway is divided into cavity cavity, tube intubation, acoustic ventilation, autonomous breathing through nose catheter or mask oxygen。
Until data are collected, it is clear that only the main adverse events leading to significant clinical consequences will be included in the combined outcome of the significant serious adverse clinical events. The composite ending is defined as one or more of the following situations: low blood pressure, after surgery, which requires the injection of an booster pump (excluding the separate use of anesthesia during anaesthesia); low oxygen saturation from the baseline, which requires clinical intervention (extended, > 1 minute), such as a continuous increase in fio2, continuous changes in ventilation strategies, changes in gastrophagus management, additional medications, or changes in surgical methods; air route upgrading management (e. G., gastrophate intulation for patients who are initially sequestered or anesthetized in a self-respiratory state); cardiac abnormalities requiring medication or electrical treatment; initiation or upgrading of vascular expansional treatment; a patient who does not require a breathing support prior to surgery, requiring a positive convulsion gas (general failure to remove a tube after an incision); and cpr, an external oxygen (ecmo) support or death within 24 hours. A review of medical records to find the combined endings during anaesthesia, as well as cpr, ecmo or death during anaesthesia or within 24 hours of anaesthesia。
Statistical analysis
Follow the guidelines for strengthening the quality of observational studies in epidemiology (strobe). Disaggregated data are expressed in terms of frequency and percentage and continuous data are expressed in terms of median and quadrant spacing. An estimate of the incidence of adverse events, 95 per cent confidence interval (ci), based on a broad range-only equation estimate (gee) model, takes into account internal relevance of the testee of the same testee. The combination effect regression analysis was used to determine the factors associated with the compound outcome of the adverse event and to consider that the same testee was repeatedly retrieved. The results are expressed in the adjusted strength ratio (aors) and the corresponding 95 per cent ci and p values. A factor of 0. 05 p in the single factor analysis is included in the multifactor analysis. Conservative p in multifactor analysis to control false positive results due to multiple tests
Result
There were 862 operations carried out by 249 children, of which 592 were cardiac catheters and 278 were non-heart surgery and diagnostic video screenings. The median age is 1. 6 years (iqr, 0. 5-8 years) and 9. 5 ibs (iqr, 5. 4 ~ 21. 2 ibs). Ph causes include left heart disease (45 per cent), left-to-right diversionary physiology (30 per cent), narrow pulmonary veins (20 per cent), primary pulmonary disease (20 per cent), speciality or primary pulmonary artery pressure (9 per cent), congenital glycerine (7 per cent) and rheumatism (1 per cent). The flow mechanics data for the heart catheter show a median of 36 mmhg (iqr, 29-48 mmhg) and 5. 1 wood units (iqr, 4-8. 3)。

Eighty-two per cent of the children who undergo a heart catheteric procedure use a whole-body anesthesia with an intubation of the tube and inhalation of heptafluoro- or hexafluoro-alkanes (84 per cent), 10 per cent self-respiration with oxygen from the nose catheter or mask, and 4 per cent use acoustic luminum under the acoustic ventilator. Forty-eight per cent of patients require positive muscle support and 14 per cent inhaled nitrogen oxide (ino) for ph (excluding those used for blood vessels only). Twenty-three per cent of patients were transferred to intensive care after a heart tube。
Patients who undergo non-heart surgery and visual examination after their first heart catheters are usually younger and underweight (median age 0. 7 v 1. 6 years, medium weight 6 v 9. 5 kg). A quarter of the cases also included gas-channel operations, such as larynx mirrors, bronchial lenses, trachea and tonsiectomy (n = 70, 25 per cent). 59 per cent of patients were fully impregnated and inhaled heptafluoro- or hexafluoro-alkanes (69 per cent), 18 per cent were self-absorbed for oxygen in nose catheters or masks, and 5 per cent were using acoustic airway devices. 31% of patients need new positive muscle support during anaesthesia and 10% receive ino treatment ph. Twenty-seven per cent of the patients were anesthetized and transferred to intensive care。
The rate of serious clinical malfeasance in heart catheter cases is 28% (95% ci, 24%-33%). Non-heart surgery is 22% (95% ci, 17%-28%). The most common adverse events are the need for positive pressure aerobics (n = 145, 17 per cent) after surgery for children who do not require respiratory support, the need for vascular infusion (n = 99, 11 per cent) after surgery for patients who do not require vascular activity support, and the apparent low oxygen haemorrhage (n = 63, 7 per cent) for clinical intervention. Multifactor analysis shows that the under-age (aor, 1. 4 years per reduction; ci, 1. 1-1. 9; p=0. 01) is an independent relevant factor in the occurrence of significant serious adverse clinical events. Operation in the heart tube operating room is associated with the increased incidence of significant adverse clinical events (aor, 5. 1; ci, 1. 7-16; p=0. 004). Operation time extension is associated with aor, 1. 3/30; ci, 1. 1-1. 4; p=0. 001. Patients with trachea are less likely to experience adverse events (aor, 0. 1; ci, 0. 04-0. 5; p=0. 001). Intervention catheters are associated with increased incidence of serious adverse events (or 2. 23; ci, 1. 5-3. 3; p)
There were four cases of the outbreak centre, two during the operation of the gas route in the main operating room and two during the operation of the catheter. Three cases were followed by hypoxiaemia during intubation or bronchial lens operation. One case of incomplete left heart development syndrome, partial pulmonary vein anisogenic flow, emergency intubation of patients after phase i of palliative surgery ecmo. The heart rate stopped 24 hours after three cases of anaesthesia. Deaths in surgery and, in one case, within 24 hours of anesthesia. The combination of death within 24 hours, ecmo or cpr compound fate regression analysis did not identify any factors associated with the patient, anaesthesia or surgery。
Conclusions
A large queue study of children diagnosed with ph through a heart catheter showed that although children in groups could be placed under guardianship and safely released from hospital to return home, there was a high risk of an adverse event during the surgery. Factors such as the age of the child, the length of the operation and the location of the heart catheter surgery are independently related to serious adverse clinical events, while pre-operative catheteric artery is less relevant to serious adverse clinical events. Compared to purely diagnostic heart catheters, the incidence of clinically significant serious adverse events involved in the catheters has almost doubled. In the management of anaesthesia of pediatric patients, the control of airways or airways, including anaesthesia induction and awakening periods, should be considered high-risk periods. In the case of young children with ph, the procedure should be carefully planned to reduce the time of anaesthesia. Further research is needed to identify and assess strategies to reduce the special risks for ph children。
Love's little drunk point:
The author presented a retrospective cross-section study of serious clinical malpractices associated with anaesthesia catheters, non-heart surgeries or visual examinations for children with hypertension. The overall incidence of adverse events in the queue was 26 per cent, which included, inter alia, the need for mechanical ventilation after the operation, the need for anaesthesia after hypotensive surgery, and the need for clinical intervention for low oxygen haemorrhage. There is a higher risk of serious adverse clinical events for young people, and the risk is reduced for every age increase. In addition, the operation and length of operation in the catheters are associated with risk factors. Compared to purely diagnostic catheters, the intervening catheters are associated with an increase in the incidence of serious adverse clinical events. As a result, ph patients need special attention and joint efforts from multidisciplinary teams, including paediatric anesthetists, cardiologists, general surgeons and paediatric cardiovascular surgeons。
The most safe method of anaesthesia for patients with ph has been the subject of constant debate, with some arguing that the aperture should be avoided, while others consider it safe to control the airways. The single-factor analysis of the study shows a correlation between anaesthesia methods and adverse events, but the multiple-factor regression shows no clear correlation between anaesthesia methods and serious adverse events. Respiratory incidents during anaesthesia continue to be a common cause of cardiac arrest in children, especially for potential heart attacks. At the same time, the period of induction and recovery of anaesthesia, as well as any other period of airway operation, should be considered a high-risk period for a respiratory event. There are cases of rapid establishment of safe airways, successful recovery without significant after-effects, as well as cases of low aerobic haematosis and/or rapid development of low ventilation to pulmonary arteries。
In addition, the study also reflected some of the pediatric anesthesiologists ' aesthetic management in patients with ph, such as sobering catheters to ensure adequate oxygen collage and ventilation, attention to adequate pain and to avoid agitation during awakening to prevent increased pulmonary vascular resistance. In the case of infants or high-risk children with unstable pulmonary vascular resistance, it is recommended that they be transferred to the care and recovery of the intensive heart ward and that nitrogen oxides be inhaled if necessary。
White, yellow, happy
Other organiserI'm sorry, but i'm sorry, but i'm sorryJ cardiothor vasc an. 2022, 36(6): 1606-1616.



