Since the advent 17 years ago of the technology to induce multi-energy stem cells (also known as ips cells or ipsc), great progress has been made in stem cell biology and regenerative medicine. Human ipsc has been widely used in disease modelling, drug detection and cytology development. New pathological mechanisms have been clarified, new medicines from ipsc screening are being developed and clinical trials using human ipsc derivatives for the first time have been initiated. In particular, the combination of human ipsc technology with recent developments in genetic editing and 3d organs has made the ipsc-based platform stronger in its various fields of application, including precision medicine。
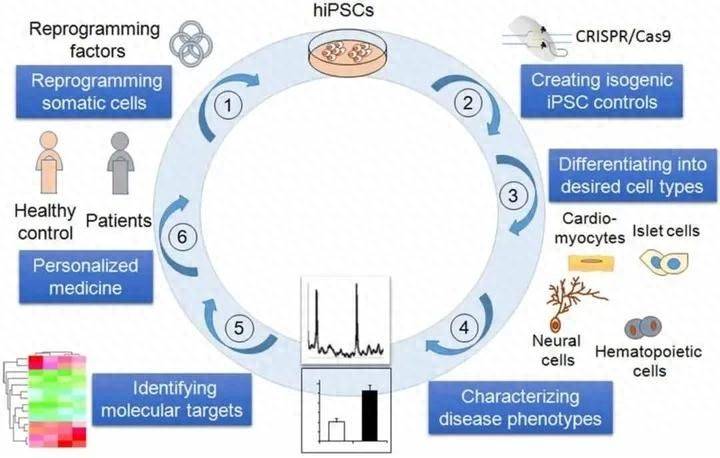
Figure 1。
Ipsc profile
For the first time in 2006, the kyoto university mountain laboratory reported the use of a mixture of four transcribing factors to produce from mice cells (e. G. Fibre cells) cells with genetic expression/show genetic characteristics and developmental potential similar to embryonic stem cells (escs), referred to as ipscs, which can be divided into three embryos (intra-, outer and meso) and four factors: oct4, sox2, klf4 and c-myc are named “yamanakaens”, collectively known as oskm. In 2007, the yamanaka team succeeded in transforming human body cells into stem cells similar to human esc (hesc), known as human ipsc (hipsc). Since then, ipsc has generated wide interest among researchers in the fields of toxicology, pathology, virology, developmental anatomy and physiology. Shinya yamanaka and sir john gurdon were also awarded the nobel prize for physiology or medicine in 2012 for “discovering that mature cells can be reprogrammed into multi-energy cells”。
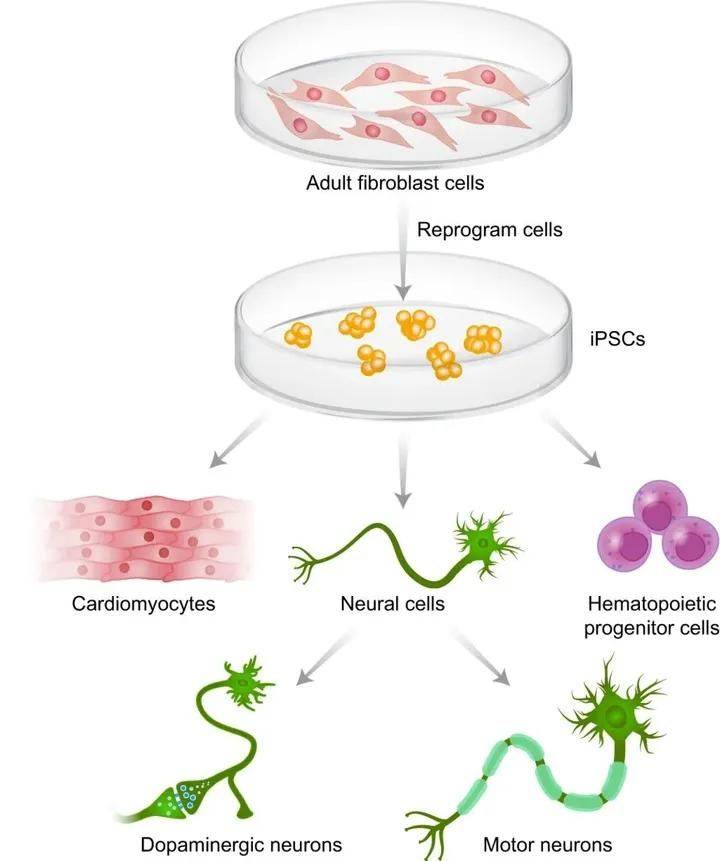
Figure 2 production and fragmentation of ipsc (borger et al., 2017)。
Until then, the path to the development of human stem cells had not been smooth as a result of the exclusion of stem cell immunity and social and ethical problems. The scientific community was heartened when ipsc was born. Unlike other sources of stem cells, ipsc successfully circumvents immuno-exclusion and ethical issues by importing four transcribing factors into mature body cells by re-coding them. The advantages of ipsc can be seen in three main ways: first, the ipsc is highly similar to human stem cells (not identical, with slight differences in performance), which can be replicated in vitro indefinitely and applied to large-scale culture; second, the ipsc can be induced to divide into needed strains based on demand, with relatively stable batch properties, avoiding inconsistencies in clinical efficacy; and third, the ipsc cells are sourced from adult cells that avoid ethical problems and are easily accessible. If ipsc is of its own origin, it can also reduce the problem of immunization exclusion. At present, however, the ipsc technology is still characterized by less efficient differentiation, risk to the safety of tumors to be verified, and the immunogenic nature of heretic induction。
Ipsc application in disease
Http://clinicaltrials. Gov
The search of https://www. Clinicaltrials. Gov/) found that there were 86 ipsc clinical trials. In 2015, the number of ipsc-related clinical trials rose significantly, peaking in 2018 and falling back. Of these, the fastest is cynata therapeutics, but most are still in the pre-clinical and pre-clinical phase i. Let's get to know the progress of the ipsc in all kinds of diseases
I. Ipsc and tumours
Embedded antigen receptor (car)-t-cell therapy has become one of the most promising treatment strategies for malignant neoplasm treatment, and six car-t-cell products have so far been approved by the united states food and drug administration (fda) for treatment of b-cell leukemia/lymphoma and multiple osteomenoma. However, patients receiving car-t-cell treatment must face a number of risks, including cytological emission syndrome (crs) and immuno-cell-related neurotoxicity syndrome (icans) and transvestite resistance to host disease (gvhd)。
The ipsc has unlimited multiplier capacity, while maintaining its multi-energy and spectroscopy potential, thus creating an ipsc bank with different combinations of pure human white cell antigens (hla), which can reduce the risk of immuno-exclusion from its own car-t cell by matching the optimal ipsc source with hla between host and moving plants. Another option is to use genetic editing to eliminate hla-i and/or hla-ii expressions. One advantage of the use of ipsc is that car-t cells can be produced from individual ipsc cloning build-up capabilities, so that the genetic modifications they experience will be homogenous in the final cell mass。
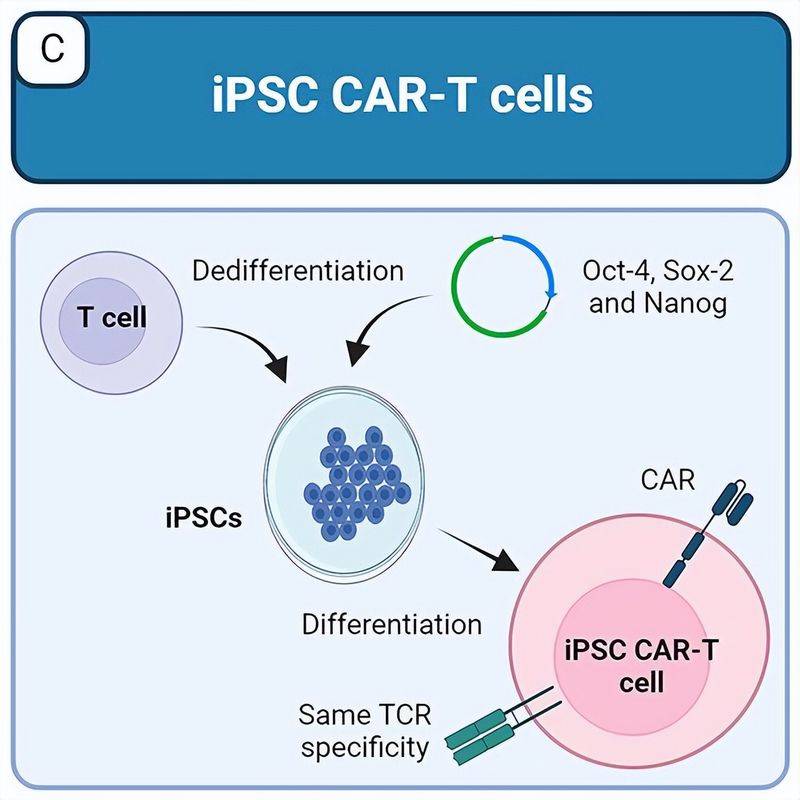
Figure 3 ipsc produces a tumour-resistant car-t cell strategy (aparcio et al., 2023)。
To address the issue of immuno-exclusion, wang et al. Developed the ipsc-derived car-t cells, which lack not only hla-i and hla-ii, but also cd 155, which encodes nk-cell activation of the receptor's dna m-1 formulation and induces hla-e expression, thus preventing nkg2a+nk cell exclusion。
Ii. Ipsc and immunological diseases
Basic research using ipsc, the source of immuno-related diseases, is expected to be a promising platform for elucidating mechanisms for the occurrence of immuno-diseases and for drug discovery. Since self-inflammatory diseases are usually monogenetic, genetic mutations affect cell function, ipsc of the patient's source tends to exhibit disease-specific appearances. In particular, ipsc-derived mononucleus and megacormic cells can be used in functional experiments. Using ipsc technology, researchers can easily access human cells and study diseases using human samples, and use ipsc to study human immuno-related diseases with clear advantages compared to traditional research methods, particularly their own immune diseases (figure 4)。
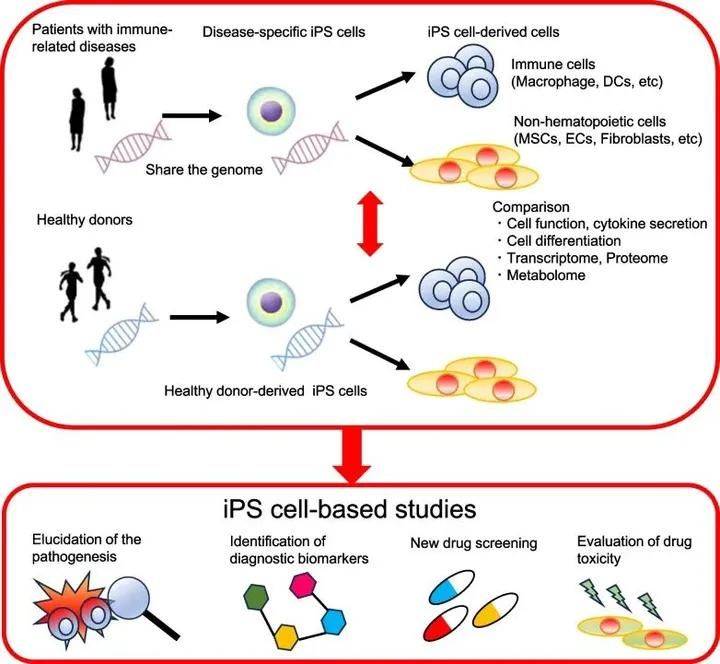
Figure 4 diagrams of immuno-related diseases using ipsc from patient sources (shoda et al., 2023)。
In order to study the mechanisms for the occurrence of immune diseases, it is essential to model in vitro diseases using cells from ipsc sources. Single nucleotodes and megacorts derived from ipsc fragmentation are often used to analyse the appearance of immuno-related diseases. Immuno-related diseases are the result of immune system disorders, in which self-inflammatory diseases are characterized by the key role played by the agitation cytokinetic factors in the onset mechanism, and sudden changes in immuno-related genes directly cause diseases, such as cyclical fever syndromes, methopathic disorders and other newly discovered single-genic inflammatory diseases. In contrast to their own inflammatory diseases, they are caused by antigen specific immuno-response disorders, such as self-immunitis, systemic red hemorrhoids (sle), rheumatism (ra), vertical spinal disease (as), pesetasis (bd), dry syndrome (ss), systemic sclerosis (ssc)。
Since auto-inflammatory diseases are usually monogenetic, ipsc of the patient's source can display a disease-related appearance, i. E. Ipsc of the patient's own inflammation disease source can be used for biomarker detection and drug screening. While autoimmune diseases are multi-genetic, the accumulation of a variety of low-impact causal variations contributes to the process of autoimmunisation and morbidity, the effects of individual risk genes are often subtle in the case of ipscs of their own sources of immuno-diseases, and the identification of pathogenic genes is a challenge, especially because of differences between ipscs of health providers and ipscs of their own sources of immune diseases. Although the mechanism for causing diseases by environmental factors is complex and difficult to replicate in vitro, ipsc-based studies can be used to assess their impact. Despite the limitations of ipsc-based research on autoimmune diseases, many high-profile studies using innovative strategies have been published。
Ipsc and nematode diseases
Celetal diseases are a group of hereditary diseases affecting any age, any organ, caused by mutation of cytological cores and linear particle genes (e. G. Linear particle dna (mt dna)), usually multisystem diseases, affecting tissues or organs with high energy demand (e. G. Nervous system, heart and skeletal muscles), as well as single organs and tissues (e. G. Ears and eyes). Currently, many ipsc models have been developed for the origin of patients with mitochondriary diseases (figure 5)。
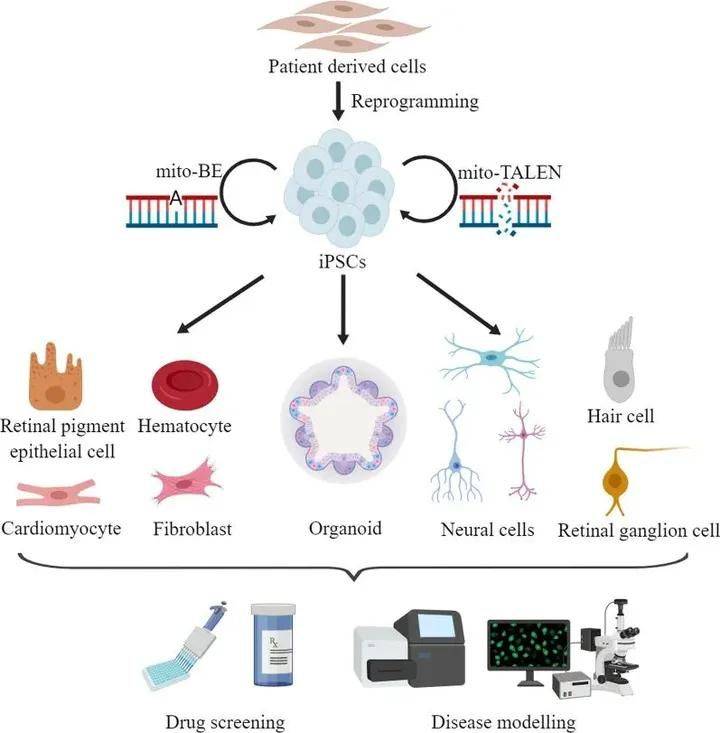
Figure 5 establishment of ipsc models (chen c and guan m x., 2023)。
It has been noted that base-based editing of mt dna in ipsc may produce mitochondriac disease models and develop potential therapeutic interventions. In fact, however, the traditional cristpr/cas system, which relies on sgrna, is incompatible with the linear particle, and in 2020 liu et al. Designed the inactivity split-ddda, which can catalyse the conversion of c. G. To t. A. From the mt dna. In 2022, kim et al. Used tale to modify deoxygendase from bacterial tada protein to catalyse the conversion of a to g and to expand the application of mt dna base editor. The combination of ipsc technology and gene editing technology will provide powerful tools for the generation of disease models and the development of effective treatment for these diseases (figure 6)。
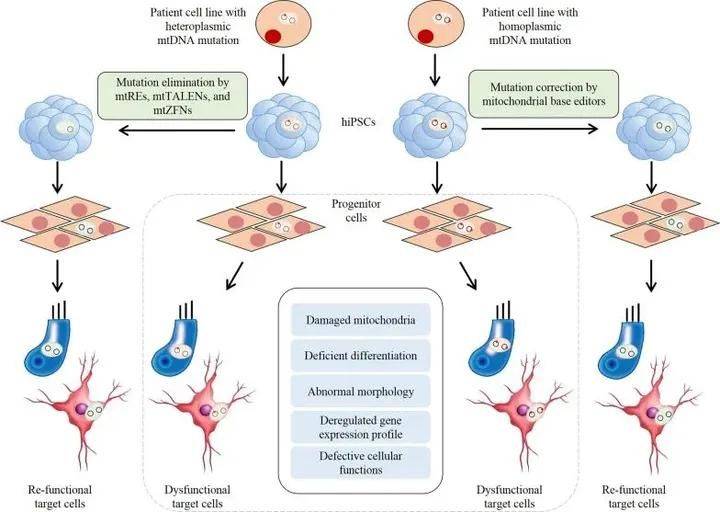
Figure 6 is a combination of ipsc and mt dna gene editing techniques (chen c and guan m x., 2023)。