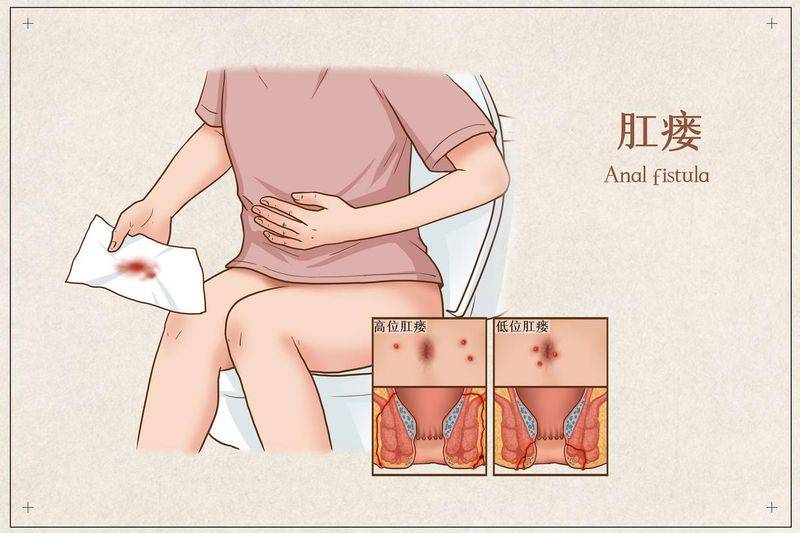
Anal fistula is one of the common diseases in the anal section. The disease can occur at any age, mostly among young men。
Type of disease reported
Anal fistula can be broken down into four categories based on its low level and number:
According to the classification of fistula in relation to slugs (parks classification), the following four categories can be classified:
Cause of death
Most of the anal fistula is caused by anesthesia around the rectal anal tube, which forms the outer body of the skin of the anus, either by self-invulsion or by cutting it open. Anal tractal diseases (e. G., cronosis, tuberculosis, ulcer colonitis, etc.), malignant neoplasms, and anal injuries can also cause anal fistula, which is relatively rare。
The abscess is self-inflicted or cut open the flow to form the external mouth, which is situated around the anal skin. The temporary closure of the external mouth, which is subject to partial inflow, re-emergence and re-emergence, re-bursts of the closed external mouth or new external vents in other locations, can result in multiple fistulas and external vents。
In addition to the above, according to the origin of the infection, anal fistula can continue to be caused by infections caused by vaginal surgery, such as post-partum suture infections, infection of the prostate, infections of the acoustic rectum, etc., infection of the acoustic rectum; diabetes, leukaemia, tuberculosis, etc., caused by blood-borne infections due to reduced physical resistance; and, in part, ulcer colonitis, crone disease, rectal anal cancer。
Prolonged spicy and greasy diets can lead to constipation or diarrhoea, increasing the incidence of anal anus and anal fistula。
Sitting, staying up, smoking and alcohol addiction, overwork are all contributing factors to anal anus and anal fistula, and prolonged sitting leads to constant high pressure in the anus, late nights, labour leading to gastrointestinal disorders, changes in defecation habits, followed by anal disease, which increases the probability of anal anus and anal fistula。
Symptoms reported
Anal fistula is mainly manifested in the continued or intermittent flow of small quantities of sepsis, blood and mucous secretions. Some of the larger high-level anal fistulas can be excreted from faeces and gas due to myocardial limitations. When fistula is healed outside, the sepsis is formed and the flow of the fistula is not smooth, the patient can feel visible pain, accompanied by symptoms of overall infection and a reduction in post-epressure symptoms. Repeated symptoms and difficulties in healing are the most important clinical characteristics of anal fistula。
When fistula is closed and sepsis is formed and fluidized, it can be accompanied by all-infection symptoms such as fever, cold fighting and inactivity。
Let's get to the doctor
In the case of repeated anal knots with ulcers, prompt medical treatment is recommended。
The doctor will make a comprehensive judgement in conjunction with the patient's complaint, the relevant medical history, symptoms, the results of the visual examination, etc. Among them, the mri test provides a clear picture of the location of fistula and its relationship with the slugs, and some patients can find their insides through mri. Mri scans are particularly important for the diagnosis and treatment of complex anal fistula。
Priority is given to anal intestinal consultations for patients with repeated anal convulsions and a small number of impulsive cortexes, with the option of general surgery in primary hospitals。
The key to anal fistula treatment lies in finding the right place within the fistula。
A small number of cases can be directly identified through anal identification. Anals can be shown by touching a cortex or dent at a tooth line, and a constricted fistula can be transmitted, i. E. An internal fistula。
Most cases of fistula are hidden, or even closed, and need to be located through the outside and along the fistula line, broken down into six methods of “seeing, touching, detecting, pouring, taking and cutting”。
On call. According to the goodsall law, the patient is stoned, a line is drawn between the anus, and if the external cavity does not exceed 5 cm before (up) or beyond the anus, the internal cavity is often straight on the anal acoustic (dental line) corresponding to the external cavity, and if the external acoustic distance is greater than 5 cm or behind (lower line), the internal cavity is convulsed many times back, and the internal cavity is often bypassed by the positive median line after the anus (6 points)。
In the case of an anus, a low anal fistula can be identified. In cases where fistula is deeply located, where fistula is not fully formed or falls within the staves, the internal location needs to be further identified。
The use of a soft probe to access the inside of a fistula, which applies to simple anal fistula, should first address cases of fistula closure, decorum, etc. The operation needs to be light, so that it does not result in false tracts and insides。
If the interior position cannot be found after the above-mentioned method, the subgal blue solution 1-2 ml may also be injected from the external mouth to determine the internal position by observing the colored part of the white veil that fills the anal tube and the lower rectum. The law also needs to be premised on fistula access。
In other words, video tools, currently more widely used than clinically, can be used by experienced physicians to determine the location, extent, relationship to and internal location of fistula. Mri is able to show more clearly where fistula is located and how it relates to muscular muscles, and to specify the location and number of internal fistulas。
If the inside location cannot be confirmed at the end, the fistula can only be removed and the inside can be searched along the side of the scar and the dead tissue。
Blood routine: regular check-ups in hospitals. Most of the symptoms of stable anal fistula have a normal blood profile, and those who suffer from a combination of acute sepsis can have an elevated blood profile。

Visual examinations (x-rays, anal cavity, mri, etc.) are used for diagnostic aids and help develop surgical programmes。
This method is used to determine the location of internal fistula and is one of the methods commonly used in clinical examinations。
When iodine oil imaging fails to identify the location of the internal fistula, it is feasible to perform a " b " check, which can clarify the location, scope, relationship to the position of the muscular and the location of the internal fistula for a less visible fistula. The high rate of positive detection helps to identify other anal diseases at an early stage。
In the case of deep-seated fistulas, it is not clear that the ultra-visibility of b is clear, and mri is able to clearly show the number, size, location and relationship of fistulas to the musculos, and some cases can be traced through mri。
In cases of complex, multi-surgery and unidentified cases of anal fistula, intestines or colonoscopy should be performed to exclude the presence of cronn's disease and ulcers。
Anal fistula needs to be identified with other anal diseases (artificial fractures, abscesses around the rectal anal tube), which can be identified by reference to typical symptoms, signs and visual tests。
Anal fractures are small ulcer formations of the whole of the skin of anal cavity below the dental line, which are characterized by “triple traction” which includes anal fractures, abdomen and fat anus nipples. Structurally, anal cracks are free of fistula, external mouths and inner-mouth structures, often associated with severe anal pains associated with defecation, which can be identified clinically with anal fractures。
It is an acute sepsis infection occurring within the soft tissue of the anal rectum or in the gaps between them, and anal fistula is a chronic manifestation of a chronic period long after its self-disruption or removal. Generally based on the history, symptoms and signs of the disease, it is not difficult to identify, and anaesthesia can be distinguished by anal ultrasound and mri scans。
Therapeutic report
Surgical surgery is the primary means of treating anal fistula and is based on the basic principles of removing stoves and fluid flow, minimizing auscultation damage and protecting anal function。
Owing to the complexity of anal fistula and some particular pathological contexts, there is a certain rate of recurrence of anal fistula. Given the importance of the particular pathological and physiological context and anal functions of high-complex fistula, the survival of fistula can also be chosen as a principle and its potential serious complications should not be overlooked in the blind pursuit of surgical treatment. The chinese medicine treatment is limited to the adjustment of the patient's recovery period and to those who are temporarily unfit for surgery。
Anal fistula is characterized by intermittent and episodic periods, with no visible symptoms, during which time it can be treated with medication for temporary relief if it is not possible to operate immediately。
The principle of surgical treatment is to cut or remove fistula and to create an open and creative face for healing. The key to the operation is to clarify the itinerary and internal location of the fistula, and doctors will minimize the auscultation damage to patients while avoiding relapse. At present, anal fistula operations consist mainly of four types。

All fistulas are removed and the scar tissues on the edges of the cut are fully removed, making the flow flow smooth and the cut healing. It applies to low-level anal fistula。
It is a method of slowly cutting anal fistula with rubber bands or medical lines. It applies to low or high levels of pure anal fistula at within 3-5 cm of the anus, either internal or external, or as an auxiliary treatment for the removal of complex anal fistula. It has the advantage of adequately protecting anal functions and reducing the risk of anal incontinence。
Fistula cutting and removing all fistula walls to healthy organizations without stitching their surfaces, which, if they are larger, can be partially stitched and partially open, is applicable to the less mature parts of a low-simplistic anal fistula or high-acrotomic fistula structures, or to the external parts of abs。
Complex anal fistula operations require a full and critical assessment of post-operative anal function and the risk of recurrence, and doctors may consider having patients live with fistula if expectations are poor。
The type of chinese medical certificate for anal fistula includes evidence of wet fever, positive inflammation certificates, vulva loss certificates, etc., and can be treated in regular medical institutions。
It is used for pre-operative and post-operative care. The hyper-wet method is used for wet thermal deposition; the venom method is used for positive inflammation; and the pyromic thermal method is used for vaginal loss certificates. The above treatment is applied in the early post-modern anal fistula period, and in the latter, in the form of a healthy temper。
These include decomposition therapy, leash therapy, fumigation, overlaying, dead herring, ligation, needle sting, induction, etc. At present, there are eight methods of extraterrestrial control that are common in clinical practice: surge flow; decomposition; scar removal tube; detoxification muscles; scabie intake; canopy; leaky muscles; and adhesive poison。
Blockage act: this act applies to the onset of simple anal fistula, where 0. 5 per cent of the body is nitrous and saline is washed and injected from the outside. While this law can be painless, the cure rate is low。
We'll be back
Anal fistula is difficult to heal and requires surgical treatment, but there is a risk of relapse after surgery. Repeated and chronic fistulas are at risk of cancer。
If the patient does not receive timely treatment or if the condition is poorly controlled, the condition of anal fistula is repeated, which eventually exhausts and results in acoustic musculos, leading to abnormality or loss of function, and even if surgical treatment is difficult to maintain normal anal function, the patient will experience abnormality or even anal incontinence. Some complex anal fistula patients also suffer from anal incontinence after surgery, with minor cases of temporary incontinence and varying degrees of permanent incontinence。
In addition, there is a risk of cancer in recurring, chronic fistula。
Prevention coverage