The field navigator
Please don't forget to make an appointment for the matriculation
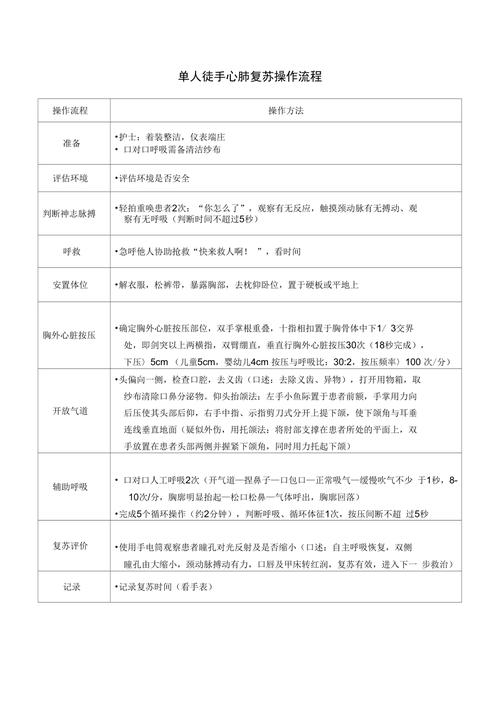
Single-person cpr operation is a very important operational technique in nursing care, and it is important that each nurse's partner has the knowledge to do the right thing. Today, the young editor brought you a single person cpr for one of the nursing operations。
Single person cpr
Operational elements:

Assessment and safety at the scene: the first-aid bai slashed the patient's shoulder and shouted, “are you okay?” to check if the patient is breathing. An emergency response system is activated without breathing or normal breathing。
2. Initiate emergency medical services, ems and obtain aed:
If the patient is found to be non-reactive and non-respiratory, the ems system is activated (telephone 120), the aed (if available), and the cpr is applied to the patient, if required, with immediate defibration。
If there are several first aid workers on the scene, one of them conducts the cpr in a step-by-step manner and the other activates the ems system (call 120) for aed。
In the case of inundation or suffocation, the first responder should first perform five cycles (2min) of the cpr and then call 120 to activate the ems system。
3. Pulse examination: for non-specialized first aid workers, emphasis is no longer placed on training to examine the pulse, and as long as a non-reactive patient is found not to be breathing autonomously, the treatment should be based on a cardiac arrest. For medical personnel, it is common to touch the carotid artery of the patient with a first-hand index finger and a middle finger. The time for the examination of pulses should normally not exceed 10 seconds, and if the presence of pulses cannot be determined within 10 seconds, the extra chest pressure should be implemented immediately。
4. Extra chest pressure (circulation, c): to ensure that the patient is lying on the ground or under his shoulder with an extra chest pressure plate, the first aider may use a different position, such as a kneeling or step-stool, to place the palm of one hand in the centre of the patient's chest, the lower half of the chest, and the other hand in the first hand. The elbow at the pressure shall be stretched straight, with a vertical downward pressure, with an adult having a pressure frequency of at least 100 times/min and a pressure depth of at least 125 px, with a complete response to the chest profile after each pressure。
At 50 per cent of the pressure time and 50 per cent of the relaxing time, the grip cannot be removed from the chest so as not to move by the pressure point. In the case of children with a single hand or both hands at the level of the nipple link, in the case of infants, both fingers are applied at the level of the titty line. In order to minimize out-of- chest pressure disruptions due to ventilation, for adults who do not have artificial air vents, the 2010 international cpr guidelines recommend a pressure-through-to-air ratio of 30:2。
For infants and children, a ratio of 15:2 is used for double-person cpr. If a double or multiple person is rescued, the cpr should be replaced every two minutes or five cycles and the conversion should be completed within five seconds, since the study shows that the operator's pressure quality begins to decline after 1 to 2 minutes of the pressure。
Open airways (airway, a): an important change in the 2010 cpr and ecc guidelines of the american heart association is the initiation of breast pressure prior to ventilation. Out of chest pressure can generate blood flow and should be minimized and interrupted throughout recovery. It takes time to reposition the head, seal the seal for mouth-to-mouth breathing, take a bag mask for artificial breathing, etc. The application of 30:2 pressure-to-pressure gas reduces the duration of the initial pressure delay compared to the start of the cpr。
6. Artificial respiration (breathing, b): before artificial respiration is given, normal inhalation is sufficient and no deep inhalation is required; all artificial breathing (whether mouth-to-mouth, mouth-to-face mask, ballbag-to-airway) should be sustained for more than one second to ensure sufficient gas inflow and a perusal; if the first artificial respiration fails to bring up the chest, it can again be used to lift the cones with a backsliding to open the airway and give a second ventilation; excessive ventilation may be harmful and should be avoided。
7. Aed defibrillation: internal tremors are the more common and easier to treat in the early stages of cardiac arrest. For vf patients, the survival rate is highest if the cpr and tremors can be implemented immediately within 3-5min of the loss of consciousness. Rapid defibrillation is a good way of treating vfs for short periods of time for patients who have a heart stop outside the hospital or who are hospitalized with a custodial heart。
Clinical performance:

The vast majority of patients suffer from no symptoms and often have a sudden onset. A small number of patients have non-specific symptoms such as dizziness, lack of strength, heart palpitation and chest suffocation from minutes to minutes before the onset of the disease. The major clinical manifestations of the sudden loss of consciousness and the disappearance of the heart and major arteries were cardiac arrest。
(b) a general heart arrest rate of 3 to 5 seconds, with the patient suffering from dizziness and black palladium; a stop time of 5 to 10 seconds caused by a lack of oxygen in the brain, i. E. A loss of consciousness; the a-s syndrome can occur in 10 to 15 seconds with full-body convulsions and incontinence; the brakes range from 20 to 30 seconds when breathing is interrupted or stopped, accompanied by pale or purple。
At 60 seconds of stopover, pupils spread out; if stoppage exceeds 4 to 5 minutes, serious irreversible damage is often caused by chronic oxygen deficiency in the central nervous system. Auxiliary examinations are most important with electrocardiograms, with some patients showing cardiac tremors within four minutes of cardiac arrest and more so in four minutes。
Please do not forget to make an appointment for the matriculation check-up。