Nursing speaker for respiratory diseases: date: purpose
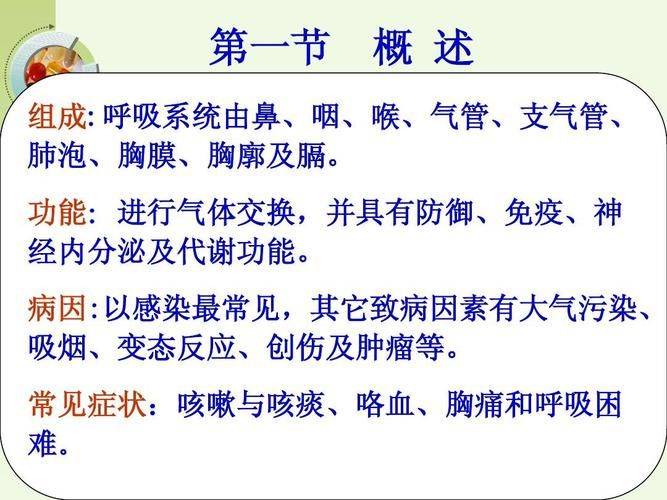
Catalogue02 assessment of respiratory disease for persons with respiratory system diseases, summary of mental care and health guidance for persons with rehabilitative system diseases, 04. The classification of respiratory diseases can be broken down into diseases of the nasal, bronchial and bronchial, pulmonary, pleural, etc., by pathogen, infectious, non-infective, obstructive, restrictive, etc. The definition relates to the occurrence of respiratory diseases, which are classified as causes of disease, to a variety of factors, including infections, physico-stimulation, allergies, genetics, etc. Risk factors such as smoking, air pollution, occupational exposure and age growth are important risk factors for respiratory diseases. The main clinical manifestations of the causes of morbidity and risk factors of respiratory diseases include cough, cough, respiratory difficulties, chest pain, etc., which can cause respiratory failure in serious cases. The diagnosis of diseases of the clinical respiratory system is based on the history of the disease, clinical performance, medical examination and relevant laboratory examinations, such as blood protocol, stinging, lung function examination, chest x-ray or ct. The high incidence of respiratory diseases, based on clinical performance and diagnosis based on preventive measures and those of critical importance, has serious implications for the health and quality of life of the population, and it is therefore important to prevent the occurrence of respiratory diseases. Prevention measures are effective against risk factors of respiratory diseases, such as smoking cessation, keeping indoor air clean, enhancing exercise and avoiding exposure to allergies. The assessment of patients with respiratory diseases02 assesses the function of the lung through indicators such as lung activity, pulmonary permeability, blood oxygen saturation, etc. Pulmonary function x-rays, cts, etc. Can detect lung pathologies and chest cavity fluids. Visual examination of the severity and duration of symptoms such as cough, cough, breathing difficulties, chest pain, etc. Laboratory examinations, such as blood routines in clinical performance assessment and haemorrhagic culture, help to determine pathogens and levels of infection. The methods and indicators used for assessing laboratory examinations assess the existence of psychological disorders such as anxiety, depression and their impact on the quality of life and dependence of treatment. Anxiety and depression are informed about the patient's family and social support and assess whether the patient receives adequate care and attention. Social support assesses patients ' attitudes, beliefs and responses to diseases and their ability to cooperate actively with treatment and care. An assessment of the psychological and social situation of the patient in response to the response, 010203, determines the type and frequency of care services needed by the patient, depending on the patient's condition and ability to provide care. Care needs are analysed for possible care problems for patients, such as respiratory difficulties, poor coughing, and lack of abdomen. Common problems assess possible complications and accidents of patients, such as respiratory failure, lung infections, etc. The analysis of potential risk care needs and problems develops individualized care measures, such as oxygen therapy, mist inhalation, body flow, etc., based on the patient's condition and needs. Targets for targeted care interventions set clear targets for the assessment of care effectiveness, such as improving respiratory function, reducing symptoms and improving quality of life. The effectiveness of care measures is regularly assessed, adjusted and optimized in the light of patient feedback and changing conditions. The individualized care programme develops measures for the care of patients with respiratory diseases,03 which maintain the use of the gravitationality method to keep the respiratory tract smooth by changing the patient's position and diverting the lung or respiratory genre in the direction of the position. The position flowing through the light patting of the patient's back, the vibration sap, which relaxes and excretes the patient, applies to patients who are unable to cough or whose sluice is not easily slurry. The water or pharmacological fluid is sent into the respiratory tract in the form of mist, by means of devices such as fogging, wetting, etc., to dilute the sapling fluid to facilitate coughing or inhaling. Back-stamping uses a slurry or straw to suck out the sluice or secretion in the patient's respiratory tract in order to keep the respiratory tract open and operate softly to avoid damage to the respiratory mucous membrane. Inhalation 01020403 hydroxytherapy in the respiratory tract selects the appropriate oxygen therapy, such as oxygen in the nose catheter, mask oxygen in order to increase the saturation of the patient's haematosis and to mitigate the symptoms of oxygen deficiency, depending on the patient's condition and degree of oxygen deficiency. Inhalation by fog sends a drug or physical salt water in the form of fog into the respiratory tract for the purposes of wetting the respiratory tract, diluting the aroma, mitigating bronchial convulsions, etc., and in the event of fogization the amount of fog is adjusted to avoid excessive irritation of the respiratory tract. The combination of oxygen therapy and mist inhalation, combined with oxygen therapy, enhances the efficacy of treatment and increases the comfort of patients. Oxygen therapy and mist inhalation techniques encourage patients to use drugs on time and on a quantitative basis, to increase drug dependence and to avoid problems such as inadequate treatment or drug poisoning. The use of medications is guided by the patient's medical conditions and characteristics, including the dose, route, time, etc., to ensure safe and effective use. The drug watch closely monitors the patient's response to the drug, including its efficacy, adverse effects, etc., and adjusts the drug programme in a timely manner to avoid serious consequences such as respiratory depression caused by the drug. Drug treatment management and detection of complications prevention and treatment strategies prevent respiratory difficulties and treat 01 to closely observe the respiratory condition of patients, detect and deal with respiratory difficulties in a timely manner and avoid serious complications such as respiratory failure. The prevention and treatment of lung infections02 strengthens the respiratory management of patients, keeping them open, preventing pathogen intrusion, and rational use of antibiotics to control the occurrence of lung infections. The prevention of heart failure and the handling of patients with respiratory diseases are prone to heart failure. Life signs such as heart rate, blood pressure, etc., should be closely observed to detect and treat the symptoms of heart failure in a timely manner to avoid deterioration. The prevention of multi-organ failure and the treatment of acute respiratory disease in 04 can lead to multi-organ failure, and monitoring and treatment should be strengthened to detect and address the symptoms in a timely manner and to improve the survival of patients. The physical functioning of patients during rehabilitation care and health guidance for respiratory diseases 04 has gradually improved, but there may still be varying degrees of symptoms such as short air and low strength. The gradual recovery of the physical function may cause psychological problems such as anxiety, depression, etc. Due to physical discomfort caused by illness, limited mobility, etc. Patients with a higher psychological burden are more sensitive to the smoke, dust, cold air, etc. In the environment, which can cause respiratory infections or increase the disease. The characterization of patients during rehabilitation is influenced by external factors, and appropriate physical exercise in the exercise of the 010203 and respiratory function is trained to develop appropriate sports programmes, such as walking, jogging, tai chi, etc., based on the patient's state of health, to improve the body's immune and cardiovascular functions. Respiratory function training of respiratory muscles guides patients to deep breathing, abdominal breathing, etc., to improve pulmonary aerobics and reduce respiratory distress. Respiratory efficiency is enhanced by the exercise of the strength and durability of respiratory muscles by simple methods such as blowing balloons and blowing candles. High-protein diets increase protein intake, such as skinny meat, fish, eggs, etc., to repair damaged respiratory tissue and improve the body's immunity. Vitamin-rich diets avoiding stimulant food nutritional support and dietary adjustment recommend more fresh vegetables and fruits to supplement nutrients such as vitamin c, vitamin a and contribute to the repair of respiratory mucous membranes and resistance to infection. Avoid eating irritated foods such as spicy, greasy, too sweet to exacerbate the inflammation of respiratory mucous membranes and the production of secretions. The involvement of family members in care encourages patients to participate in organizations or activities for the rehabilitation of respiratory diseases, exchange experiences with patients, encourage and support each other and improve the quality of life. Professional guidance and follow-up services for the establishment of social support networks should provide professional rehabilitation guidance and follow-up services, keep abreast of changes in patients ' condition and provide individualized rehabilitation advice. Families should be actively involved in the rehabilitation of patients, provide psychological support and live care, and help them build confidence against disease. Families ' participation and social support networks build psycho-care and communication skills for patients with respiratory disease 05 often generate anxiety and fear due to respiratory difficulties, repeated cases, etc. As a result of the disease, anxiety and fear may lead patients to feel dependent and vulnerable to vulnerability. People who are dependent and vulnerable have expectations for treatment and care, and hope to alleviate symptoms and restore health as soon as possible. The psychological needs of those who expect and need them are recognized and listened to with great attention, understanding their inner world and avoiding interruption or denial. Listening skills express the same sense of clarity through responses and feedback, so that patients feel understood and cared for and communicate more effectively. The interpretation of medical terms and treatment programmes in simple and clear language ensures that patients can understand them accurately. Effective communication skills teach patients how to properly conduct deep breathing and relax training to ease stress and anxiety. The technique of deep breathing and relaxing leads patients to actively deal with illness and to express internal stress by communicating with others, writing journals, etc. Psychological guidance ensures sufficient sleep and rest time and helps restore physical and mental health. The sleeping and rest stress mitigation method 01 provides information and knowledge to families about patients ' condition, treatment programmes and prognosis, helping them to understand the disease and alleviate their fears. The family psychological support strategy2 encourages participation in encouraging family participation in the care and rehabilitation of patients and in the development of treatment programmes to enhance patient confidence. Psychological support is provided to look after the emotional changes in the family, to provide timely comfort and encouragement and to reduce their psychological burden。a summary of reflections and future prospects06 has led to a significant increase in the recovery rate of persons with respiratory diseases through scientific care methods and effective treatment. The rate of patient rehabilitation has significantly improved the continuous improvement of care processes and standards and the professionalism and quality of care. The quality of care continues to improve, actively communicating with patients, paying attention to their needs, making them feel warm and caring and increasing their satisfaction. Patient satisfaction increases the outcome of this care by recalling that part of the caregiver's expertise and care skills for respiratory diseases are not sufficiently solid and require training and learning. Patient education and health education are not sufficiently sensitive to patients ' awareness of respiratory diseases and prevention, and there is a need to strengthen health education and improve patient self-management capabilities. The quality and efficiency of care services need to be enhanced by cumbersome care processes, resulting in inefficient care work, which needs to be further optimized and more efficient. There are problems and improvements in the direction of exploring scientific ways and means of implementing evidence-based care practice of 0203, finding evidence of optimal care, guiding clinical care and improving its quality and effectiveness. The application of smart care equipment will play an increasingly important role in the care of respiratory diseases, such as smart aerosols, respiratory surveillance systems, etc., as technology develops. The promotion of the concept of personalized care provides individualized care programmes for different patients, such as comprehensive care for different symptoms and needs of the patient, such as diet, exercise and psychology. New skills